
The Endocrine Interface — Pituitary and Thyroid
Fourth in a Series Summarizing the Academic Works of Redacted Science

[Welcome reader. This is the fourth in a series of articles summarizing the Redacted Science academic writings. The technical papers are available, but these summaries are made more accessible to that everyone can understand the science I am explaining]
Two organs, one architecture.
Start here if you want to start at the beginning.
→ Paper A: Candida albicans as a Biochemical Computer
This is the fourth installment in the series walking through the Redacted Science Research Initiative — sixteen peer-citable preprints, plus the Architect Reports, in the order they should be read. Each post is the Summary for the Reader from the Architect — a plain-English entry point — followed by where to find the full paper. Technical terms are unpacked in italic brackets where they appear. The Architect’s asides are in there too. You’ll know them when you see them.
Paper A described the machine. Paper B told the human origin story. Pan-Mammalian showed the architecture isn’t ours alone. This paper takes that architecture and points it at two specific organs that mainstream medicine has already documented as sites of fungal involvement — without ever asking why.
Summary for the Reader from the Architect
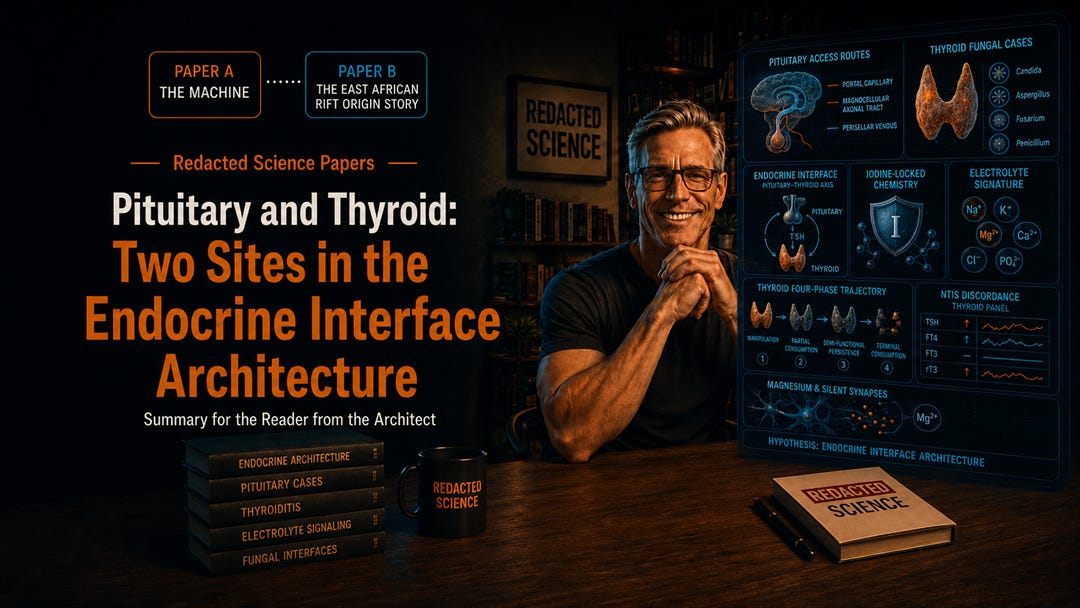
Two organs, one architecture. The pituitary and the thyroid sit at the regulatory center of mammalian endocrine function, and both have been documented as sites of fungal involvement across decades of mainstream case literature. This paper does not propose those documented cases. It reorganizes them.
The anchors are not speculative. Three culture-proven cases of Candida pituitary infection in immunocompetent hosts — Heary 1995, Strickland 2018, Chin 2021 — sit alongside a multi-genus catalog of fungal thyroiditis spanning aspergillus, candida, pneumocystis, cryptococcus, and histoplasma (Bhattacharya 2021), and a documented bidirectional electrolyte signature under fungal load and antifungal pressure (Lionakis 2008). [The framework didn’t manufacture these cases. They are sitting in the mainstream literature, indexed under “rare incidental events” because the standard pathogenesis frame has nowhere else to put them.] The Redacted Science framework reads this same evidence as the visible catalog of an integrated endocrine interface architecture.
At the pituitary, three anatomical access routes — portal capillary, magnocellular axonal tract, perisellar venous — carry organism interfacing into the gland. Each route produces a different clinical signature. Each signature matches one of the three documented cases. [The framework makes a prediction on routes. There is most certainly A route, and these appear to be the best candidates.] A multiplexing prediction extends Kex2-family processing of pituitary prohormones from prior framework work, building on Thomas 1988 and Bourbonnais 1994.
At the thyroid, the argument is sharper. Iodine-locked chemistry makes the gland biochemically hostile to fungi generically — all fungi, not just Candida. Yet the literature documents multi-genus fungal thyroiditis spanning at least five different genera. [Hostile environments do not invite five different genera. The multi-genus pattern is the diagnostic signature: this is not random opportunism, this is architectural.] Perfusion-target explanation cannot account for it. The architectural reading can: the thyroid is an interface site that the integrated organism-host architecture is positioned to use.
The thyroid four-phase trajectory follows: manipulation, partial consumption with hormone modulation, semi-functional persistence in cardiac-governance role, and terminal consumption as coordinated weakening. This trajectory maps onto the canonical course of fungal thyroiditis as it appears in the literature, with each documented case slotting into one of the four phases.
The semi-functional persistence phase is where the framework’s pieces click together. The Paper B managed-heart architecture predicts a transitional period during which thyroid output is repurposed for cardiac governance before terminal consumption. The clinical literature documents exactly such a period in long-course fungal thyroiditis.
Non-Thyroidal Illness Syndrome — the discordance signature documented in fungal sepsis (Silva 2016) — is predicted to appear at chronic-state Candida presentations. It currently doesn’t because the screening method systematically fails to capture it: TSH-only thyroid panels are blind to NTIS by design. [Same pattern as Paper A’s specific electrolyte levels, same pattern as creatinine-based eGFR in muscle wasting. The signal the framework predicts is exactly the signal the standard panel was modified to stop reporting.]
A neural-circuit extension follows. Silent synapse architecture is gated by NMDA channel magnesium, with synaptic magnesium availability tracking systemic magnesium dynamics the partnership architecture regulates (Slutsky 2010). The prediction is direct: under antifungal pressure, magnesium dynamics shift, silent synapses unlock, and cognitive function changes in the direction patients have been describing for decades. [Patients have been telling their doctors that antifungal treatment cleared their brain fog. The framework gives the mechanism. The mechanism explains why it works, why it works fast, and why it sometimes regresses when antifungal pressure is removed.]
Thirteen distinct falsification clauses are presented across levels of methodological tractability. The most tractable test requires no novel methodology and no new patient enrollment: chronic-state thyroid panel measurement in chronic Candida populations. The data exist. The cohorts exist. The tests are standard. The framework is testable today.
This paper is published openly during the longitudinal subject’s continuing observation of their own case. The architectural reading developed here is offered as the structural account that the subject’s continuing experience asks for and that the broader patient population currently lacks. [The author is broadcasting this experience and the science it generates in near real-time. Don’t expect everything to be perfect... but it is a lot closer than you are now.]
Pituitary and Thyroid: Two Sites in the Endocrine Interface Architecture Craddock, J. — 44 references DOI: 10.5281/zenodo.20060491
The full preprint, with all thirteen falsification clauses and the neural-circuit extension, is on Zenodo at the link above. CC BY 4.0.
Next in the Series
Chronic Disease as Stuck Program Modes. The umbrella paper. The framework so far has built the machine, the origin story, the clade, and the architecture at specific organs. The next move is the big one: a new disease category. The proposal is that the biochemical computer runs phased programs, and a chronic disease is what happens when one of those phases gets stuck on. Five conditions get worked out in companion papers: type 2 diabetes, anorexia, IBS, obesity, and Parkinson’s. The umbrella paper introduces the model, the selection rules, and the single measurable variable that should predict severity and treatment response across all of them.
Subscribe to get the Umbrella paper in your inbox.
— #TheArchitect
[Please share this publication so that more might know]