
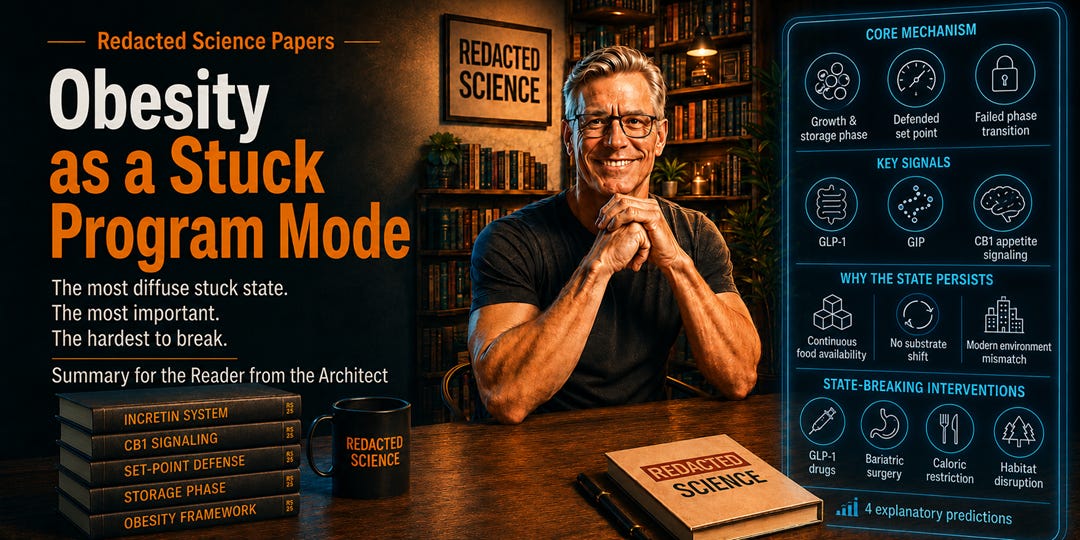
Obesity as a Stuck Program Mode
The most diffuse stuck state. The most important. The hardest to break.

[Welcome readers. Today we have the second of the nine conditions which I tied to Candida albicans. This one doesn’t seem like an illness, but I think that as a stuck-program mode, it more than qualifies. ]
Start here if you want to start at the beginning.
→ Paper A: Candida albicans as a Biochemical Computer
This is the seventh installment in the series walking through the Redacted Science Research Initiative — sixteen peer-citable preprints, plus the Architect Reports, in the order they should be read. Each post is the Summary for the Reader from the Architect — a plain-English entry point — followed by where to find the full paper. Technical terms are unpacked in italic brackets where they appear. The Architect’s asides are in there too. You’ll know them when you see them.
T2D was the cleanest mechanistic case. Obesity is the opposite — multiple signaling channels running simultaneously, no single anchor point, a defended equilibrium your body fights to maintain. It is also the stuck mode that has reorganized the modern world. Read on.
Summary for the Reader from the Architect
If type 2 diabetes is the cleanest stuck mode, obesity is the most diffuse — and the most important. [Over 1 billion people worldwide. 95% weight regain within five years. That isn’t insufficient willpower; that is a defended equilibrium.]
The standard model says you ate too much, moved too little, and now your body is storing the excess. The stuck-program model says the body is doing exactly what it was told to do — and it was told to do it by the organism. [Growth and storage phase. One of the normal operating modes in the ancestral program. It was supposed to end.]
The mechanism runs through three channels: the incretin system [the gut hormones GLP-1 and GIP that tell the pancreas when to release insulin and tell the brain when to feel full — the Ozempic target], the endocannabinoid system [CB1 receptors specifically — the same receptors cannabis activates, which is why stoners get the munchies; the organism can drive similar appetite signals without cannabis], and metabolic state assessment through GLP-1 itself. The modern environment never delivers the substrate shift that ends the storage phase, so the phase keeps running. [Forever. Until you die of it, or until something breaks the cycle.]
This is a version conflict: an ancestral program refined for Homo candidus running inside a modern host whose environment no longer supplies the signals the program expects. The framework resolves the set-point problem [why your body fights weight loss like you’re starving, even when you aren’t], explains why bariatric surgery works so dramatically [habitat disruption — rearrange the real estate the organism lives in] and why GLP-1 drugs work [sensing-channel override — you’re hijacking the signal the organism uses], and explains the post-1970s epidemic onset through antibiotic-era mycobiome disruption. [Kill off the bacteria that compete with Candida and guess who has more room to run.]
Five testable predictions are presented.
Obesity as a Stuck Program Mode of the Candida albicans Biochemical Computer Craddock, J. — 9 references DOI: 10.5281/zenodo.19600443
The full preprint, with all five testable predictions and the three-channel mechanism, is on Zenodo at the link above. CC BY 4.0.
Next in the Series
Anorexia Nervosa as a Stuck Program Mode. Anorexia has the highest mortality rate of any psychiatric disorder — higher than depression, higher than schizophrenia, higher than bipolar. Relapse rates after weight restoration run 30 to 50%. Current theory cannot explain why. The framework can. Whatever was broken stays broken after the weight comes back, because the disruption isn’t downstream of starvation — starvation is downstream of the disruption.
Subscribe to get the Anorexia paper in your inbox.
— #TheArchitect